 2018, Vol. 32
2018, Vol. 32 

2. 北京大学医药管理国际研究中心, 北京 100191
2. International Research Center for Medicinal Administration, Peking University, Beijing 100191, China
世界卫生组织(World Health Organization,WHO)指出不合理用药是世界范围内存在的问题,全世界有超过一半的药品处方、调剂或销售不合理[1]。数据显示,不合理用药是美国排名前十的死亡原因之一[2]。在中国,不合理用药形势更加严峻,医疗机构含抗生素或注射剂处方比例远高于WHO推荐标准[3],基层门诊抗菌药的处方比例为50.3%、上呼吸道感染抗菌药的处方比例高达83.7%[4],60%的儿童耳聋和脑损伤与不合理用药相关[5]。
促进合理用药需要及时准确的监测和评价,而科学的工具是评价的基础。本文通过检索中国知网、万方、Pubmed和Proquest等数据库,对有关合理用药评价的文献进行归纳、分析,综述国内外合理用药的评价工具和方法,帮助研究者构建标准化的评价体系,旨在提高药物治疗的安全性、有效性和合理性,以期对临床实践起到一定的指导作用。
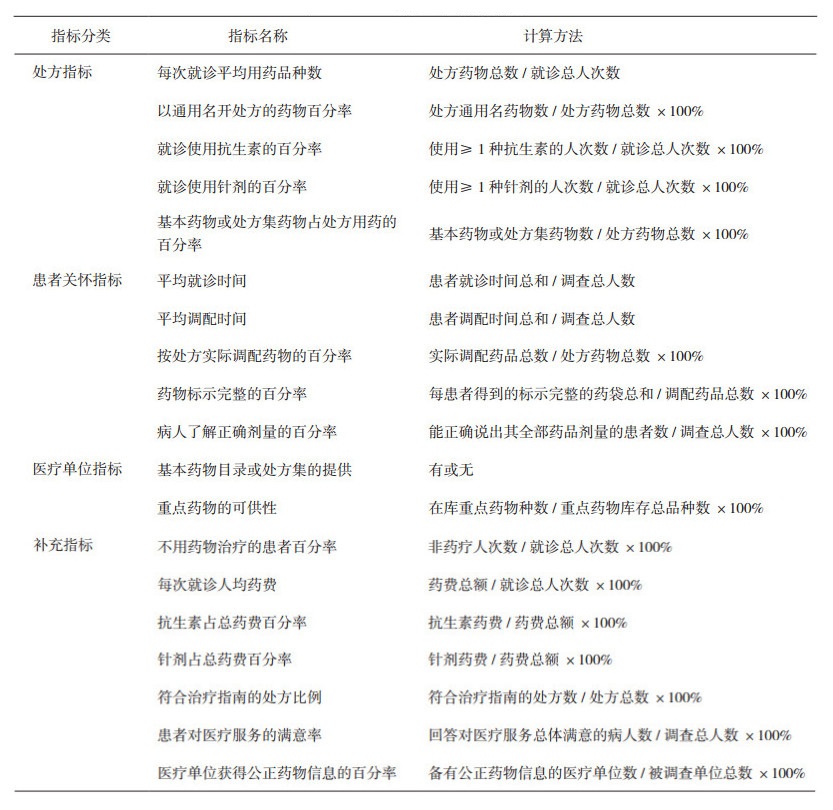
1 宏观标准 1.1 WHO不合理用药指标(WHO,1993)WHO基本药物行动计划委员会1993年制定的《医疗机构用药调查指南》提供了一种简单明确的合理用药评价方法[6]。该指标是国内外最常用的评估指标,已在40多个国家使用[7]。国内研究一般用处方指标和补充指标作为数据分析指标,而患者关怀指标与机构指标因其主观人为因素,一般作为参考或者背景数据进行分析[8]。WHO不合理用药指标的优点在于指标值可在机构、地区甚至国家间进行比较[6-7],指标及其计算方法见表 1。
|
|
表 1 WHO不合理用药指标内容 |
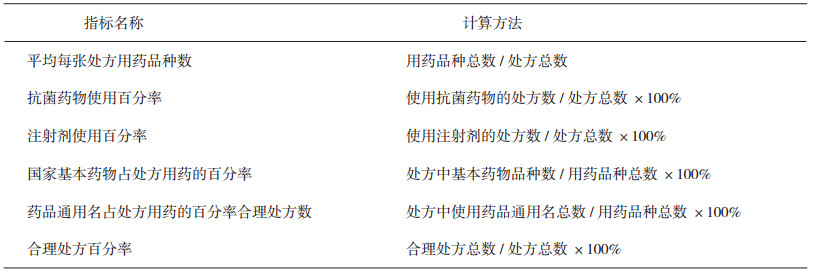
原卫生部2010年发布的《医院处方点评管理规范(试行)》规定了医院处方点评工作的评价指标。在对WHO不合理用药指标进行删减和修改的同时,该指标还需要医生或药师凭借个人知识判断“不合理处方”。不合理处方包括不规范处方、用药不适宜处方和超常处方[9]。处方点评综合考虑医生用药、患者情况等多方面因素,是判断合理用药的最准确方法。但同时,处方点评需要专业的医生或药师进行,且耗时较长,故难以应用于大量处方的评估。指标及其计算方法见表 2。
|
|
表 2 《医院处方点评管理规范》指标内容 |
在需要对大量处方进行微观评价时,可应用潜在不适当处方(potentially inappropriate prescribing, PIP)评价标准。PIP是不符合指南的次优用药行为[10],即医生处方的药物有其他更安全有效替代药物或疗法来治疗相同疾病[11],可导致更高的死亡率、更多的住院和不良反应[12]。PIP包括潜在性不适当用药(potentially inappropriate medications, PIMs)和潜在处方遗漏(potential prescribing omissions, PPOs)。评价时可以直接将有≥1个PIP的药物治疗认定为不合理用药[13],也可以每个PIMs和PPOs得1分,最后计总分。有研究[14]表明,PIP评分下降0.5可使患者因药物相关住院的风险降低17%。同时,将PIP用药审核作为一项干预措施也能够显著提高药物治疗合理性[15-16],降低老年人的用药和不良反应风险。
PIP评价有多种广泛使用的工具,根据指标特征,通常将其分为需要凭借个人知识判断的隐含式(implicit)标准和不需判断可直接回答的明确(explicit)标准[11]。
2.1 明确标准1)Beers标准(美国,1991)
Beers标准是最早也是目前应用最广泛的老年人PIMs标准,是由美国加利福尼亚大学的Mark Beers在1991年组织专家共同制定的≥65岁老年人PIMs列表[17]。经过1997、2003、2012和2015年的4次修订,Beers(2015年版)主要包括5个药物列表:①老年人潜在不适当用药;②可加剧老年人疾病/综合症的药物-疾病或药物-综合症潜在不适当用药标准;③需在老年人中谨慎使用的潜在不适当用药标准;④需在老年人中避免使用的潜在临床重要非抗感染药的用药标准;⑤需要根据肾功能调整剂量的药物[18]。Beers标准提出后,日本(2003)、德国(2010)、澳大利亚(2012)等国均对Beers标准进行了本土化[11],也有很多学者对Beers标准进行改编,创造出Laroche标准(法国,2007)、Maio标准(意大利,2010)[19]等几十种评价标准。由于标准中的很多药品在中国没有上市或已经淘汰,同时标准中的一些药物是否为老年人绝对避免使用尚有待商榷,故标准提出初期在中国的应用较少,近几年在中国学者的研究中应用逐渐增多[20-21]。
2)STOPP/START标准(爱尔兰,2008)
老年人不适当处方筛查工具(screening tool of older persons' prescriptions,STOPP)和处方遗漏筛查工具(screening tool to alert to right treatment,START)为爱尔兰Cork大学附属医院组织专家制定的筛选工具,是欧洲应用最广泛的≥65岁老年人PIP标准之一。第二版STOPP标准(2014年版)针对PIMs,包含61条常见的老年人PIMs,按系统分为10大类,每一条都注明了在特定疾病状态下使用某类药物是否适当。START标准(2014年版)针对PPOs,列出了22条可能被特定患者群体忽略的药物治疗方案[22]。STOPP/START标准除对用药中的潜在不合理情形进行分析外,还涵盖潜在处方遗漏,多项研究表明STOPP标准比同期的Beers标准更加敏感[23],中国也有很多学者将Beers和STOPP/START标准同时使用进行潜在不适当用药分析[24-25]。
3)ACOVE标准(美国,1999)
虚弱老年人治疗评估标准(assessing care of vulnerable elders,ACOVE)是美国兰德公司1999年提出的一系列老年人治疗的质量评估指标,是目前最全面系统的老年医疗质量指标[26]。ACOVE-1中将“虚弱老年人”定义为≥65岁且两年内具有较高的死亡和丧失功能风险(虚弱老年评分VES-13≥3)的老年人群[27]。但由于VES-13评估需要当面询问患者相关问题,程序相对复杂,故ACOVE-3(2006年版)将标准的适用人群改为所有≥75岁老年人。ACOVE-3包括26个专题392项指标,其中涉及药物的使用有98项[26]。有研究[28]对372个患者进行ACOVE评分发现,得分高于均值的患者比低于均值的患者3年生存率高10%。目前,国内ACOVE相关研究大多仅对指标进行介绍,鲜有单独应用。
4)中国老年人疾病状态下潜在不适当用药初级判断标准(中国,2014)
张晓兰等[29]综合多国老年PIM判断标准,通过德尔菲法建立中国老年人疾病状态下潜在不适当用药初级判断标准。最终A级标准包括35种(类)药物在25种疾病状态下的62个用药风险点,B级标准包括9种(类)药物在9种疾病状态下12个用药风险点。边原等[30]运用上述标准进行评价,发现23.1%的老年患者门诊处方存在PIMs。
5)其他明确PIP标准
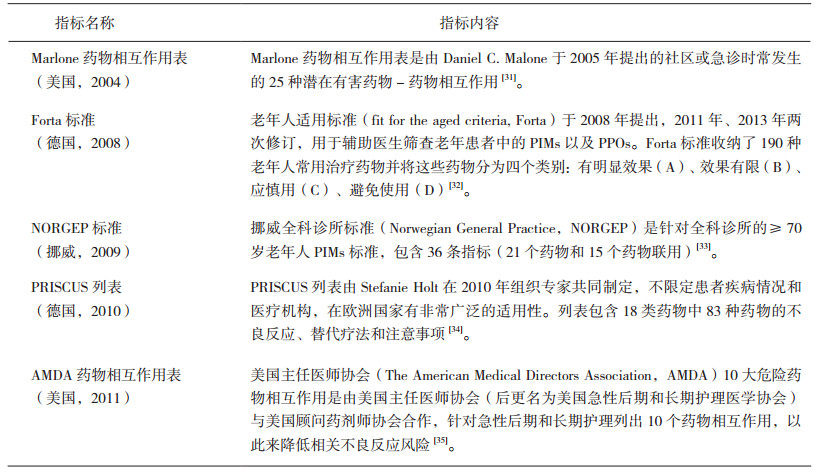
国际上有数百种PIP评价标准,在国外的研究中常见多种指标联合使用来比较不同标准的PIP检出率,提高测量准确性。本文选择了5种常见的PIP指标进行展示,指标内容见表 3。
|
|
表 3 其他明确PIP标准 |
1)处方优化方法(荷兰,2009)
处方优化方法(prescribing optimization method,POM)是由A. Clara Drenth-van Maanen等人在2009年制定的用于辅助全科医生优化老年人多药物治疗的方法。POM以6个问题作为专题,每个问题下提供了详细的评价标准。6个问题包括:①治疗是否不足以及是否有补充治疗?②患者对药物治疗的依从性如何?③哪些药可以去除或哪些药不合适?④有哪些不良反应?⑤可预测的药物-药物或药物-食物相互作用有哪些?⑥剂量和(或)剂型是否应该调整?相较于其他评价标准,该方法最大的特点在于能够帮助全科医生快速有效地减少在老年人药物治疗过程中的药物治疗不足,利用POM可使医生正确决策的比例上升13.4%[36]。
2)药物合理指数(美国,1992)
药物合理指数(medicine appropriateness index,MAI)是由Hanlon等人在1992年提出,1997年修改的标准,最早应用于65岁以上老年人,但是现在也可以用于所有住院及门诊患者的处方评价。MAI包括:①药物的适应证;②药物作用;③正确剂量;④用药指导;⑤存在临床意义的药物-药物相互作用;⑥存在临床意义的药物-疾病相互作用;⑦用药方案的可行性;⑧重复用药;⑨恰当的疗程;⑩医疗费用[16]。专家对每个项目进行评分,药物和患者均可以作为分析单位,将每个药物分数相加可得到患者得分。研究者可自行定义总分的区间,将药物的使用分为“适当”“比较适当”或“不适当” [37]。此方法适用于各种药物、临床条件和环境,最适用于在住院评价中监测处方随时间的改善[38]。但是同其他隐含式标准一样,MAI需要熟练的临床医生和药师操作且耗时。有研究[40]表明,每个药物的MAI评估平均需要10 min[39],评估每个患者的平均时间长达30 min。
3 小结不合理用药是世界范围内存在的严重问题,科学适宜的工具是及时准确评价的基础。国内外对于合理用药评价方法的研究也取得了很大成果,根据评价对象将评价方法分为宏观标准和微观标准。微观标准中,根据应用时是否需要医师、药师参与为明确标准和隐含标准;根据评价目的分为PIMs标准和PPOs标准;根据标准内容分为处方指标、患者指标、机构指标等等(见表 4)。
|
|
表 4 合理用药评价方法总结 |

不合理用药是全世界共同面临的严重问题,如何科学有效地对“不合理”进行评价也是国内外学者的研究重点。宏观标准的优点在于指标简单直观,且指标值可在机构、地区甚至国家间进行比较。微观标准可以单独使用,也可以多种指标联用[13]。微观明确标准可以在临床信息和个人数据不足的情况下,筛选数据库中的潜在不合理用药,为指导临床实践提供数据支持;微观隐含标准可以辅助医生或药师为具体患者优化药物治疗方案。无论是宏观还是微观标准都是很好的处方评价工具,但研究者在实际应用中需要关注每个标准中指标设置的理由和建议,根据不同指标的特点,充分考虑评价对象、数据特征、药品目录、地区用药习惯等因素,对于评价工具进行选择和调整。
| [1] |
The Pursuit of Responsible Use of Medicines: Sharing and Learning from Country Experiences[EB/OL]. [2017-09-21]. http://www.who.int/medicines/areas/rational_use/en.
|
| [2] |
Mao W, Vu H, Xie Z, et al. Systematic Review on Irrational Use of Medicines in China and Vietnam[J]. PLoS One, 2015, 10(3): e0117710. DOI:10.1371/journal.pone.0117710 |
| [3] |
Gong Y, Yang C, Yin X, et al. The Effect of Essential Medicines Programme on Rational Use of Medicines in China[J]. Health Policy Plan, 2016, 31(1): 21-27. DOI:10.1093/heapol/czv008 |
| [4] |
Li J, Song X, Yang T, et al. A Systematic Review of Antibiotic Prescription Associated with Upper Respiratory Tract Infections in China[J]. Medicine (Baltimore), 2016, 95(19): e3587. DOI:10.1097/MD.0000000000003587 |
| [5] |
Li Y, Xu J, Wang F, et al. Overprescribing in China, Driven by Financial Incentives, Results in Very High Use of Antibiotics, Injections, and Corticosteroids[J]. Health Aff(Millwood), 2012, 31(5): 1075-1082. |
| [6] |
World Health Organization. How to Investigate Drug Use in Health Facilities: Selected Drug Use Indicators[EB/OL]. [2017-11-16] http://apps.who.int/iris/bitstream/10665/60519/1/WHO_DAP_93.1.pdf.
|
| [7] |
唐镜波, 袁进. 基本药物-基本医疗卫生服务-合理用药的实践与依存性[J]. 中国药房, 2010(12): 1065-1069. |
| [8] |
Yao Q, Liu C, Ferrier JA, et al. Urban-rural Inequality Regarding Drug Prescriptions in Primary Care Facilities-a pre-post Comparison of the National Essential Medicines Scheme of China[J]. Int J Equity Health, 2015(14): 58-62. |
| [9] |
卫生部. 卫医管发[2010] 28号关于印发《医院处方点评管理规范(试行)》的通知[S]. 2010.
|
| [10] |
Formiga F, Vidal X, Agustí A, et al. Inappropriate Prescribing in Elderly People with Diabetes Admitted to Hospital[J]. Diabet Med, 2016, 33(5): 655-662. DOI:10.1111/dme.12894 |
| [11] |
Kaufmann C P, Tremp R, Hersberger K E, et al. Inappropriate Prescribing:a Systematic Overview of Published Assessment Tools[J]. European Journal of Clinical Pharmacology, 2014, 70(1): 1-11. DOI:10.1007/s00228-013-1575-8 |
| [12] |
Spinewine A, Schmader K E, Barber N, et al. Appropriate Prescribing in Elderly People:How Well Can it be Measured and Optimised?[J]. Lancet, 2007, 370: 173-184. DOI:10.1016/S0140-6736(07)61091-5 |
| [13] |
Wallerstedt S M, Belfrage B, Fastbom J. Association Between Drug-specific Indicators of Prescribing Quality and Quality of Drug Treatment:a Validation Study[J]. Pharmacoepidemiol Drug Saf, 2015, 24(9): 906-914. DOI:10.1002/pds.v24.9 |
| [14] |
Haag JD, Davis AZ, Hoel RW, et al. Impact of Pharmacist-Provided Medication Therapy Management on Healthcare Quality and Utilization in Recently Discharged Elderly Patients[J]. Am Health Drug Benefits, 2016, 9(5): 259-268. |
| [15] |
O'Mahony D, Gallagher P, Ryan C, et al. STOPP & START Criteria:a New Approach to Detecting Potentially Inappropriate Prescribing in Old Age[J]. European Geriatric Medicine, 2010, 1(1): 45-51. DOI:10.1016/j.eurger.2010.01.007 |
| [16] |
苏培, 徐静, 郎奕. 处方的评价方法和评价工具[J]. 药品评价, 2010(12): 17-20. DOI:10.3969/j.issn.1672-2809.2010.12.005 |
| [17] |
李影影, 邢玉晶, 王烨, 等. Beers标准和STOPP/START标准再评价老年住院患者医嘱点评情况[J]. 药学与临床研究, 2016(1): 57-60. |
| [18] |
Radcliff S, Yue J, Rocco G, et al. American Geriatrics Society 2015 Updated Beers Criteria for Potentially Inappropriate Medication Use in Older Adults[J]. Journal of the American Geriatrics Society, 2015, 63(11): 2227-2246. DOI:10.1111/jgs.13702 |
| [19] |
Rognstad S, Brekke M, Fetveit A, et al. Prescription Peer Academic Detailing to Reduce Inappropriate Prescribing for Older Patients:a Cluster Randomised Controlled Trial[J]. Br J Gen Pract, 2013, 63(613): 554-562. DOI:10.3399/bjgp13X670688 |
| [20] |
Mo L, Ding D, Pu SY, et al. Patients Aged 80 Years or Older are Encountered More Potentially Inappropriate Medication Use[J]. Chin Med J(Engl), 2016, 129(1): 22-27. |
| [21] |
边原, 蔡璐璐, 龙恩武, 等. Beers标准2015版在住院老年患者不适当用药评价中的应用[J]. 中国新药与临床杂志, 2016, 35(10): 751-758. |
| [22] |
O'mahony D, O'sullivan D, Byrne S, et al. STOPP/START Criteria for Potentially Inappropriate Prescribing in Older People:Version 2[J]. Age Ageing, 2015, 44(2): 213-218. |
| [23] |
Gallagher P, Lang PO, Cherubini A, et al. Prevalence of Potentially Inappropriate Prescribing in an Acutely Ill Population of Older Patients Admitted to Six European Hospitals[J]. Eur J Clin Pharmacol, 2011, 67(11): 1175-1188. DOI:10.1007/s00228-011-1061-0 |
| [24] |
Li H, Pu S, Liu Q, et al. Potentially Inappropriate Medications in Chinese Older Adults:The Beers Criteria Compared with the Screening Tool of Older Persons' Prescriptions Criteria[J]. Geriatrics & Gerontology International, 2017, 17(11): 1951-1958. |
| [25] |
周海峰, 沈杰, 纪芳, 等. Beers标准联合STOPP/START准则评价我院内科老年住院患者潜在不适当用药[J]. 中国药房, 2016(23): 3212-3214. |
| [26] |
Wenger NS, Roth CP, Shekelle P. ACOVE Investigators. Introduction to the Assessing Care of Vulnerable Elders-3 Quality Indicator Measurement set[J]. J Am Geriatr Soc, 2007, 55(2): 247-252. |
| [27] |
Saliba D, Elliott M, Rubenstein L Z, et al. The Vulnerable Elders Survey:a Tool for Identifying Vulnerable Older People in the Community[J]. Journal of the American Geriatrics Society, 2001, 49(12): 1691-1699. DOI:10.1046/j.1532-5415.2001.49281.x |
| [28] |
Higashi T, Shekelle P G, Adams J L, et al. Quality of Care is Associated with Survival in Vulnerable Older Patients[J]. Ann Intern Med, 2005, 143(4): 274-281. DOI:10.7326/0003-4819-143-4-200508160-00008 |
| [29] |
张晓兰, 王育琴, 闫妍, 等. 中国老年人疾病状态下潜在不适当用药初级判断标准的研制[J]. 药物不良反应杂志, 2014(2): 79-85. |
| [30] |
边原, 李刚, 杨勇, 等. 采用潜在不适当用药初级判断标准评价门诊老年患者的用药合理性[J]. 中国新药与临床杂志, 2015, 34(1): 68-72. |
| [31] |
Malone D C, Armstrong E P, Abarca J, et al. Identification of Serious Drug-drug Interactions:Results of the Partnership to Prevent Drug-drug Interactions[J]. J Am Pharm Assoc(2003), 2004, 44(2): 142-51. DOI:10.1331/154434504773062591 |
| [32] |
Kuhn-Thiel A M, Weiß C, Wehling M. Consensus Validation of the FORTA(Fit for The Aged)List:a Clinical Tool for Increasing the Appropriateness of Pharmacotherapy in the Elderly[J]. Drugs & Aging, 2014, 31(2): 131-140. |
| [33] |
Rognstad S, Brekke M, Fetveit A, et al. The Norwegian General Practice(NORGEP)Criteria for Assessing Potentially Inappropriate Prescriptions to Elderly Patients:a Modified Delphi Study[J]. Scandinavian Journal of Primary Health Care, 2009, 27(3): 153-159. DOI:10.1080/02813430902992215 |
| [34] |
Holt S, Schmiedl S, Thürmann PA. Potentially Inappropriate Medications in the Elderly:the PRISCUS List[J]. Dtsch Arztebl Int, 2010, 107(31-32): 543-551. |
| [35] |
Top 10 Particularly Dangerous Deug Interactions in Pa/ltc[EB/OL]. [2017-09-21]. http://www.paltc.org/top-10-particularly-dangerous-drug-interactions-paltc.
|
| [36] |
Drenth-van Maanen A C, van Marum R J, Knol W, et al. Prescribing Optimization Method for Improving Prescribing in Elderly Patients Receiving Polypharmacy[J]. Drugs & Aging, 2009, 26(8): 687-701. |
| [37] |
Lodato F, Poluzzi E, Raschi E, et al. Appropriateness of Proton Pump Inhibitor(PPI)Prescription in Patients Admitted to Hospital:Attitudes of General Practitioners and Hospital Physicians in Italy[J]. European Journal of Internal Medicine, 2016(30): 31-36. |
| [38] |
Muth C, Harder S, Uhlmann L, et al. Pilot Study to Test the Feasibility of a Trial Design and Complex Intervention on Prioritising Multimedication in Multimorbidity in General Practices(PRIMUMpilot)[J]. BMJ Open, 2016, 6(7): e011613. DOI:10.1136/bmjopen-2016-011613 |
| [39] |
Buetow S A, Sibbald B, Cantrill J A, et al. Appropriateness in Health Care:Application to Prescribing[J]. Social Ccience & Medicine, 1997, 45(2): 261-271. |
| [40] |
Alassaad A, Melhus H, Hammarlund-Udenaes M, et al. A Tool for Prediction of Risk of Rehospitalisation and Mortality in the Hospitalised Elderly:Secondary Analysis of Clinical Trial Data[J]. BMJ Open, 2015, 5(2): e007259. DOI:10.1136/bmjopen-2014-007259 |